Repaglinide(瑞格列奈)
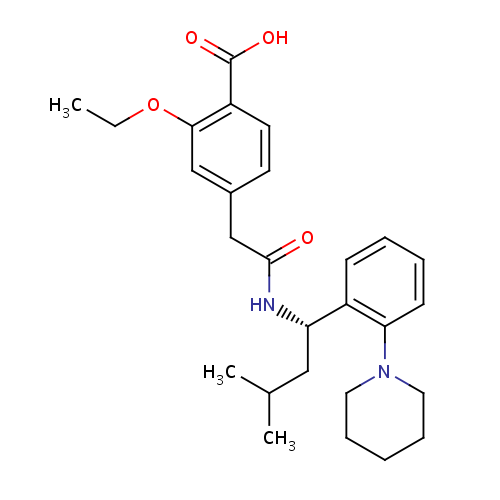
Monoisotopic: 452.26750765
Repaglinide is an oral antihyperglycemic agent used for the treatment of non-insulin-dependent diabetes mellitus (NIDDM). It belongs to the meglitinide class of short-acting insulin secretagogues, which act by binding to β cells of the pancreas to stimulate insulin release. Repaglinide induces an early insulin response to meals decreasing postprandial blood glucose levels. It should only be taken with meals and meal-time doses should be skipped with any skipped meal. Approximately one month of therapy is required before a decrease in fasting blood glucose is seen. Meglitnides may have a neutral effect on weight or cause a slight increase in weight. The average weight gain caused by meglitinides appears to be lower than that caused by sulfonylureas and insulin and appears to occur only in those naïve to oral antidiabetic agents. Due to their mechanism of action, meglitinides may cause hypoglycemia although the risk is thought to be lower than that of sulfonylureas since their action is dependent on the presence of glucose. In addition to reducing postprandial and fasting blood glucose, meglitnides have been shown to decrease glycosylated hemoglobin (HbA1c) levels, which are reflective of the last 8-10 weeks of glucose control. Meglitinides appear to be more effective at lowering postprandial blood glucose than metformin, sulfonylureas and thiazolidinediones. Repaglinide is extensively metabolized in the liver and excreted in bile. Repaglinide metabolites do not possess appreciable hypoglycemic activity. Approximately 90% of a single orally administered dose is eliminated in feces and 8% in urine.
- Novo nordisk inc
- Novo Nordisk Inc.
- Boehringer Ingelheim Ltd.
- Cardinal Health
- Kaiser Foundation Hospital
- Lake Erie Medical and Surgical Supply
- Novo Nordisk Inc.
- Recipharm AB
| Synthesis Reference | Not Available |
| General Reference |
|
| Type | small molecule |
| Classes |
|
| Substructures |
|
| Indication | As an adjunct to diet and exercise to improve glycemic control in adults with type 2 diabetes mellitus. | ||||||||||||
| Pharmacodynamics | Insulin secretion by pancreatic β cells is partly controlled by cellular membrane potential. Membrane potential is regulated through an inverse relationship between the activity of cell membrane ATP-sensitive potassium channels (ABCC8) and extracellular glucose concentrations. Extracellular glucose enters the cell via GLUT2 (SLC2A2) transporters. Once inside the cell, glucose is metabolized to produce ATP. High concentrations of ATP inhibit ATP-sensitive potassium channels causing membrane depolarization. When extracellular glucose concentrations are low, ATP-sensitive potassium channels open causing membrane repolarization. High glucose concentrations cause ATP-sensitive potassium channels to close resulting in membrane depolarization and opening of L-type calcium channels. The influx of calcium ions stimulates calcium-dependent exocytosis of insulin granules. Repaglinide increases insulin release by inhibiting ATP-sensitive potassium channels in a glucose-dependent manner. | ||||||||||||
| Mechanism of action | Repaglinide activity is dependent on the presence functioning β cells and glucose. In contrast to sulfonylurea insulin secretatogogues, repaglinide has no effect on insulin release in the absence of glucose. Rather, it potentiates the effect of extracellular glucose on ATP-sensitive potassium channel and has little effect on insulin levels between meals and overnight. As such, repaglinide is more effective at reducing postprandial blood glucose levels than fasting blood glucose levels and requires a longer duration of therapy (approximately one month) before decreases in fasting blood glucose are observed. The insulinotropic effects of repaglinide are highest at intermediate glucose levels (3 to 10 mmol/L) and it does not increase insulin release already stimulated by high glucose concentrations (greater than 15 mmol/L). Repaglinide appears to be selective for pancreatic β cells and does not appear to affect skeletal or cardiac muscle or thyroid tissue. | ||||||||||||
| Absorption | Rapidly and completely absorbed following oral administration. Peak plasma concentrations are observed within 1 hour (range 0.5-1.4 hours). The absolute bioavailability is approximately 56%. Maximal biological effect is observed within 3-3.5 hours and plasma insulin levels remain elevated for 4-6 hours. When a single 2 mg dose of repaglinide is given to healthy subjects, the area under the curve (AUC) is 18.0 - 18.7 (ng/mL/h)^3. | ||||||||||||
| Volume of distribution | 31 L following IV administration in healthy individuals |
||||||||||||
| Protein binding | >98% (e.g. to to albumin and α1-acid glycoprotein) | ||||||||||||
| Metabolism |
Repaglinide is rapidly metabolized via oxidation and dealkylation by cytochrome P450 3A4 and 2C9 to form the major dicarboxylic acid derivative (M2). Further oxidation produces the aromatic amine derivative (M1). Glucuronidation of the carboxylic acid group of repaglinide yields an acyl glucuronide (M7). Several other unidentified metabolites have been detected. Repaglinide metabolites to not possess appreciable hypoglycemic activity.
Important The metabolism module of DrugBank is currently in beta. Questions or suggestions? Please contact us.
|
||||||||||||
| Route of elimination | 90% eliminated in feces (<2% as unchanged drug), 8% in urine (0.1% as unchanged drug) | ||||||||||||
| Half life | 1 hour | ||||||||||||
| Clearance | 33-38 L/hour following IV administration |
||||||||||||
| Toxicity | LD50 >1 g/kg (rat) (W. Grell) | ||||||||||||
| Affected organisms |
|
||||||||||||
| Pathways |
|
||||||||||||

| Properties | |||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| State | solid | ||||||||||||||||||||||||||||||||||||||||||
| Experimental Properties |
|
||||||||||||||||||||||||||||||||||||||||||
| Predicted Properties |
|
||||||||||||||||||||||||||||||||||||||||||
| Drug | Interaction |
|---|---|
| Acebutolol | Acebutolol may decrease symptoms of hypoglycemia and increase the time required for the body to compensate for hypoglycemia. |
| Atenolol | The beta-blocker, atenolol, may decrease symptoms of hypoglycemia. |
| Betaxolol | The beta-blocker, betaxolol, may decrease symptoms of hypoglycemia. |
| Bevantolol | The beta-blocker, bevantolol, may decrease symptoms of hypoglycemia. |
| Bisoprolol | The beta-blocker, bisoprolol, may decrease symptoms of hypoglycemia. |
| Carteolol | The beta-blocker, carteolol, may decrease symptoms of hypoglycemia. |
| Carvedilol | The beta-blocker, carvedilol, may decrease symptoms of hypoglycemia. |
| Clarithromycin | Clarithromycin may increase the effect of repaglinide. |
| Cyclosporine | Cyclosporine may increase the therapeutic and adverse effects of repaglinide. |
| Erythromycin | The macrolide, erythromycin, may increase the effect of repaglinide. |
| Esmolol | The beta-blocker, esmolol, may decrease symptoms of hypoglycemia. |
| Fluvastatin | Inhibitors of CYP3A4 and P-glycoprotein may increase serum concentrations of repaglinide. Monitor concomitant therapy closely. |
| Gemfibrozil | Gemfibrozil may increase the effect and toxicity of repaglinide. |
| Glucosamine | Possible hyperglycemia |
| Josamycin | The macrolide, josamycin, may increase the effect of repaglinide. |
| Labetalol | The beta-blocker, labetalol, may decrease symptoms of hypoglycemia. |
| Metoprolol | The beta-blocker, metoprolol, may decrease symptoms of hypoglycemia. |
| Nadolol | The beta-blocker, nadolol, may decrease symptoms of hypoglycemia. |
| Oxprenolol | The beta-blocker, oxprenolol, may decrease symptoms of hypoglycemia. |
| Penbutolol | The beta-blocker, penbutolol, may decrease symptoms of hypoglycemia. |
| Pindolol | The beta-blocker, pindolol, may decrease symptoms of hypoglycemia. |
| Practolol | The beta-blocker, practolol, may decrease symptoms of hypoglycemia. |
| Pravastatin | Substrates of organic anion transporters may increase levels of repaglinide. Monitor concomitant therapy closely. |
| Propranolol | The beta-blocker, propranolol, may decrease symptoms of hypoglycemia. |
| Rifampin | Rifampin decreases the effect of repaglinide |
| Sotalol | The beta-blocker, sotalol, may decrease symptoms of hypoglycemia. |
| Telithromycin | Telithromycin may reduce clearance of Repaglinide. Consider alternate therapy or monitor for changes in the therapeutic/adverse effects of Repaglinide if Telithromycin is initiated, discontinued or dose changed. |
| Timolol | The beta-blocker, timolol, may decrease symptoms of hypoglycemia. |
| Voriconazole | Voriconazole, a strong CYP3A4 inhibitor, may increase the serum concentration of repaglinide by decreasing its metabolism. Monitor for changes in the therapeutic and adverse effects of repaglinide if voriconazole is initiated, discontinued or dose changed. |
- Take up to 30 minutes before meals.
- When taken with a high-fat meal, AUC and Cmax decreases.